The State of US COVID Data: A Reality Check
As of 2023, the United States has largely abandoned comprehensive COVID-19 surveillance, leaving citizens without critical data to assess their risk. This document explains what happened, what remains, and why it matters.
Timeline of Data Dismantling
May 11, 2023: The Turning Point
- Public Health Emergency declaration ended
- Hospital reporting became voluntary (was mandatory)
- CDC COVID Data Tracker discontinued
- Most federal funding for testing ended
What We Lost
| Data Type | Before May 2023 | After May 2023 | Impact |
|---|---|---|---|
| Case Counts | Daily reporting from all states | Minimal testing, no systematic reporting | Cannot track infection rates |
| Hospital Data | Mandatory daily reporting | Voluntary, sporadic | Cannot assess healthcare strain |
| Deaths | Timely reporting | Weeks to months delayed | Cannot track mortality trends |
| Testing | Widespread availability | Minimal, mostly private | No population-level data |
| Genomic Surveillance | Robust variant tracking | Severely reduced | Limited variant detection |
| Vaccination | Detailed breakthrough tracking | Limited data | Cannot assess vaccine effectiveness |
What Remains Available
1. Wastewater Surveillance (Primary Source)
- Endpoint:
https://data.cdc.gov/resource/2ew6-ywp6.json - Coverage: ~40% of US population
- Updates: Weekly
- Reliability: High (virus RNA doesn't lie)
- Limitation: Doesn't capture individual infections
2. Limited State Reporting
States Still Reporting (with varying quality):
- California
- Minnesota
- Massachusetts
- North Carolina
- Washington
Most States: Little to no public data
3. International Comparisons
Countries with better tracking:
- UK: Comprehensive surveillance continues
- Denmark: Detailed genomic tracking
- Singapore: Weekly MOH updates
- Japan: Sentinel surveillance
The Hidden Reality
Current Infection Estimates (from wastewater)
Based on wastewater percentiles:
- >80th percentile: 2-4% of population actively infected
- 60-80th: 1-2% infected
- 40-60th: 0.5-1% infected
- <40th: <0.5% infected
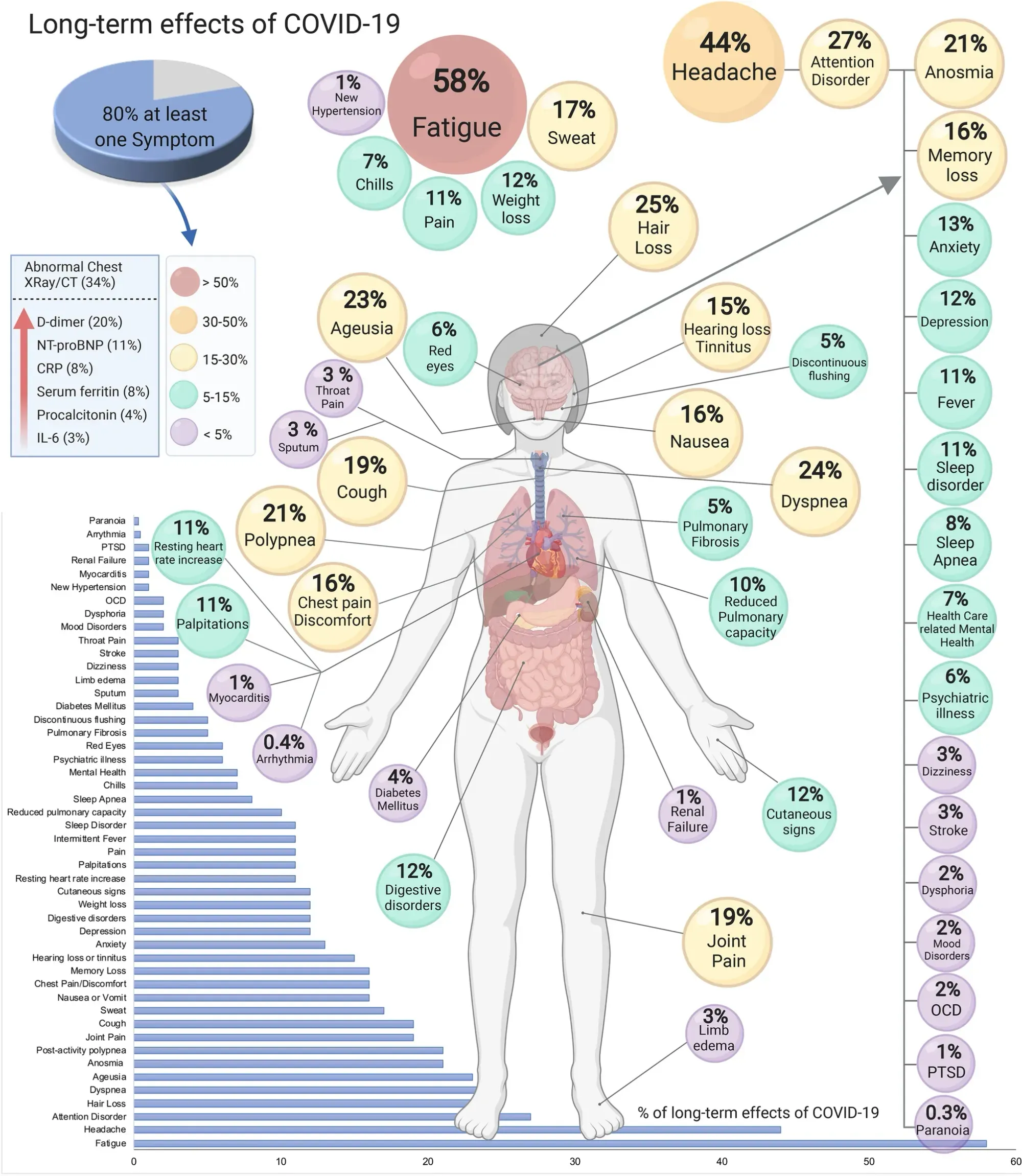
Long COVID: The Ignored Crisis
- 30-36% of COVID infections result in long COVID
- 14+ million Americans currently affected
- No cure or reliable treatment
- Cumulative risk with each reinfection
- All ages affected, including children
Annual Deaths (Estimated)
- 2024: ~47,000 deaths (no longer in top 10 causes)
- Context: Still more than car accidents
- Undercount: Likely significant due to reduced testing
Why Data Was Discontinued
Official Reasons Given
- "Emergency phase is over"- a complete lie
- "Transition to endemic management" - even though endemic in this case means it is continuously present in the population in relatively stable numbers. This is extremely flawed logic
- "Resources needed elsewhere" - anybody have any clue where?
- "Similar to flu surveillance" - another lie
Likely Additional Factors
- Economic pressure to "return to normal"
- Political fatigue with pandemic measures
- Healthcare industry lobbying
- Avoiding liability for ongoing transmission
- Money line must go up
The False Equivalence with Flu
COVID is NOT like the flu:
- Higher transmission rate
- Long COVID has no flu equivalent
- Year-round transmission (no seasonal pattern)
- More organ systems affected
- Higher mutation rate
Alternative Data Sources
Community-Driven Initiatives
- People's CDC (peoplescdc.org)
- Weekly "Weather Reports"
- Community risk assessments
- Advocacy for better data
- Independent Researchers
- Dr. Lucky Tran (@luckytran)
- Dr. Eric Topol (@EricTopol)
- Mike Hoerger (PMC COVID Tracker)
- Biobot Analytics
- Commercial wastewater monitoring
- Some public data available
What You Can Track
- Wastewater levels in your area
- Anecdotal reports from healthcare workers
- International data for comparison
- Pharmacy sales of COVID tests
- School absence rates
The Implications
For Individuals
- Cannot assess personal risk accurately
- No warning of surge periods
- Blind to variant emergence
- Long COVID risk remains hidden
For Public Health
- Cannot respond to outbreaks effectively
- No early warning system
- Variant surveillance compromised
- Resource allocation becomes guesswork
For Society
- False sense of security from lack of data
- Continued transmission without awareness
- Growing disabled population from long COVID
- Economic impacts hidden but accumulating
What Needs to Happen
Immediate Needs
- Restore mandatory hospital reporting
- Fund widespread wastewater surveillance
- Provide free testing with reporting
- Track long COVID systematically
- Resume genomic surveillance
Long-term Requirements
- Independent public health data infrastructure
- Legal protections for data transparency
- Pandemic preparedness funding
- Long COVID research and treatment
- Indoor air quality standards
How to Use Limited Data
Risk Assessment Framework
Given data limitations, consider:
Higher Risk Situations:
- High wastewater levels (>60th percentile)
- Crowded indoor spaces
- Poor ventilation
- Unmasked gatherings
- Healthcare settings
Protective Measures Still Work:
- N95/KN95 masks
- Ventilation/filtration
- Testing when available
- Vaccination (reduces severe outcomes)
- Avoiding crowds when feasible
Personal Data Tracking
Keep your own records:
- Exposure events
- Symptoms (even mild)
- Test results
- Vaccination dates
- Recovery timeline
The Bottom Line
What We Know
- COVID continues circulating year-round
- Long COVID affects 1 in 3 infections
- Wastewater shows ongoing transmission
- Many countries track better than the US
- The virus continues evolving
What We Don't Know
- Exact infection rates
- Current variants circulating
- True mortality numbers
- Healthcare system strain
- Long-term societal impact
The Cruel Irony
We have less data during the endemic phase when personal risk assessment is most critical.
Call to Action
For Individuals
- Assume transmission is occurring
- Protect yourself based on your risk tolerance
- Share information with others
- Support community tracking efforts
- Advocate for data transparency
For Healthcare Workers
- Report what you're seeing
- Track patterns in your practice
- Educate patients about ongoing risks
- Advocate for surveillance
- Document long COVID cases
For Policymakers
- Restore comprehensive surveillance
- Fund public health infrastructure
- Mandate transparent reporting
- Support long COVID research
- Prepare for future pandemics
Resources
Data & Tracking
- CDC NWSS: https://www.cdc.gov/nwss
- People's CDC: https://peoplescdc.org
- Biobot: https://biobot.io
- PMC Tracker: https://pmc19.com/data/
Information
- Your Local Epidemiologist: https://yourlocalepidemiologist.substack.com
- Eric Topol's Ground Truths: https://erictopol.substack.com
- Death Panel Podcast: https://www.deathpanel.net
Advocacy
- Marked By COVID: https://markedbycovid.com
- Long COVID Justice: https://longcovidjustice.org
- Be A Hero: https://beaherofund.org
International Data
- UK Dashboard: https://coronavirus.data.gov.uk
- Denmark SSI: https://covid19.ssi.dk
- Our World in Data: https://ourworldindata.org/covid-cases
Conclusion
The systematic dismantling of COVID surveillance in the US represents a profound failure of public health policy. Citizens are being asked to make personal risk assessments without data, while a mass disabling event (long COVID) continues largely unmeasured and unaddressed.
The virus didn't disappear when we stopped counting. The risk didn't decrease when we stopped reporting. Long COVID didn't stop when we stopped tracking.
This dashboard exists because our institutions failed us. It uses what little data remains to provide some visibility into ongoing transmission. But it shouldn't have to exist. We deserve better. We deserve transparency. We deserve data.
Stay safe. Stay informed. Demand better.